Is decarbonising what already exists enough?
Note :
The hypotheses and results presented here are taken from the SHIFT PROJECT report ‘Decarbonising health for sustainable healthcare’, in its 2nd version published in April 2023. The report and all the accompanying documents are publicly available online at the following address:
https://theshiftproject.org/article/decarboner-sante-rapport-2023/https://theshiftproject.org/article/decarboner-sante-rapport-2023/
Decarbonisation roadmap for the healthcare sector
The roadmap proposed by the SHIFT PROJECT in its report includes both cross-sectoral measures and measures by emissions category, as presented in the Bilan Carbone. The aim is to reduce emissions from the healthcare sector by 80% by 2050, in line with the requirements of the Paris Agreement, in order to achieve carbon neutrality.
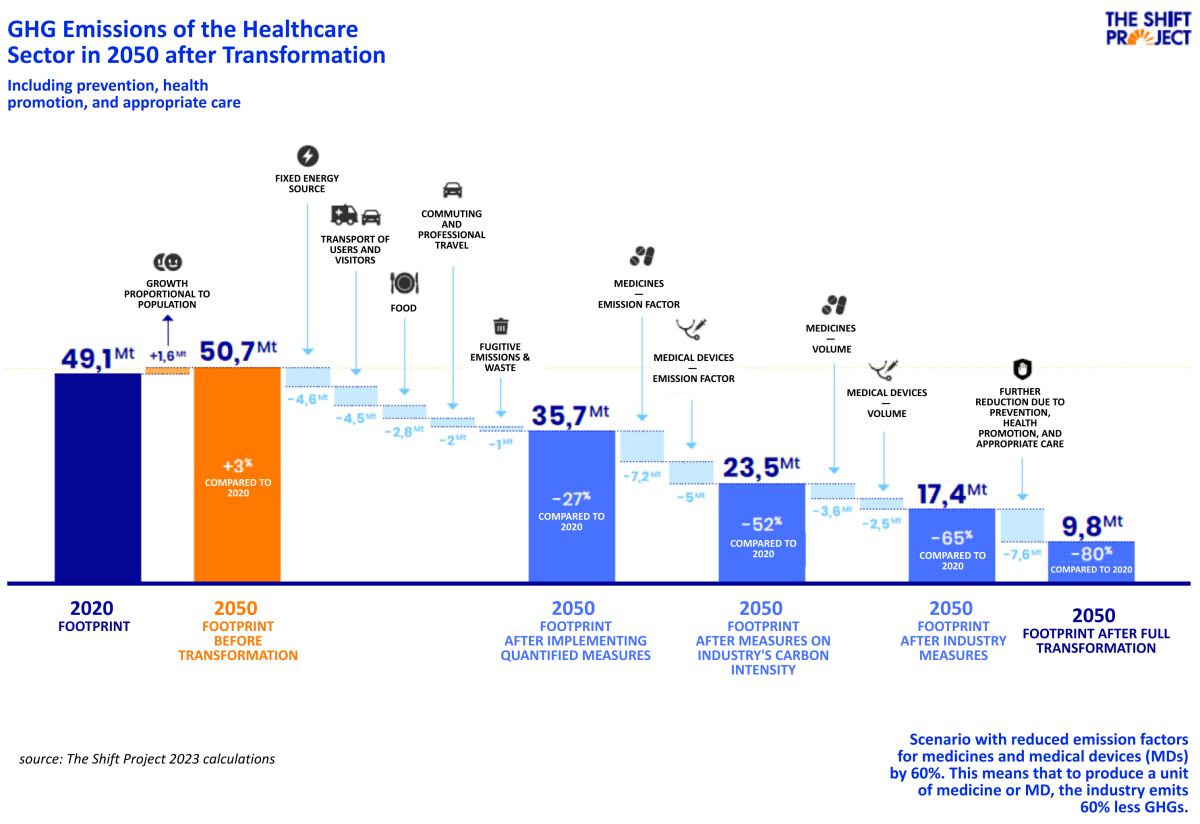
Taking into account demographic growth and the increase in demand for care, the sector's emissions before transformation will be 50.7 million tonnes of CO2eq in 2050. An 80% reduction would limit these emissions to 9.8 million tonnes of CO2eq.
The diagram below illustrates the expected reduction in emissions for each item after application of the roadmap measures. These are detailed in the following paragraphs of this chapter.
Measures ‘quantified by real data'
For each of the emission items (travel, purchasing, energy/non-energy and waste), there is sufficient knowledge and data available on their potential for reducing GHG emissions to be able to put a figure on them. These measures, to be implemented as soon as possible, have been designed with a view to reducing greenhouse gas emissions by 5% per year.
Buildings (-85% of emissions associated with energy consumption, i.e. 4.6 MtCO2e)
The proposed measures are as follows:
Massify the comprehensive, high-performance thermal renovation of hospital and medico-social buildings.
Systematically switching from gas- and oil-fired heating and/or hot water production systems to low-carbon energy sources.
Encourage bio-air conditioning of buildings and the use of bio-sourced materials in new buildings.
Organise and promote energy-saving practices.
Recruit, train or call on the skills of an energy consultant.
Train healthcare professionals to reduce usage/consumption.
Travel (-94% taking into account the electrification of vehicles, i.e. 6.5 MtCO2eq)
The proposed measures are as follows:
Co-construct, draw up and implement a mobility plan for the health or medico-social establishment or group.
Promote active mobility (cycling and walking).
Encourage the use of public transport.
Encourage car-sharing (guaranteeing the return home in the event of exceptional circumstances, setting up a car-sharing service, etc.).
Facilitate the use of teleworking for administrative staff and researchers.
Replace combustion-powered vehicles (ambulances, VSL, etc.) with electric vehicles, giving priority to second-hand vehicles where possible.
Limit the distances travelled for training courses and conferences: develop e-learning and local conferences accessible by train.
Develop telemedicine for consultations that can be treated as tele-expertise.
Where medical conditions allow, encourage patients to be grouped together for medical transport.
Food (-48% of emissions from food purchases, i.e. 2.8 MtCO2e)
The proposed measures are as follows:
Reduce food waste by improving the taste and dietary quality of meals.
Systematically offer vegetarian meals sourced locally and in season. Substitute some animal proteins with vegetable proteins (particularly in the case of beef).
Reduce the amount of packaging and the omnipresence of plastic in mass catering.
Fugitive emissions (-75% of emissions from medical gas purchases, i.e. 0.4 MtCO2e)
The proposed measures are as follows:
Ban high-greenhouse gas anesthetics.
Encourage the use of inhalers with low environmental impact (e.g. dry powders or mist).
Waste (-14% of waste emissions, i.e. -0.07 MtCO2e)
The proposed measures are as follows:
Supporting the development of production in France and the use of reusable medical equipment/devices.
Develop recycling channels for single-use devices.
Reduce the proportion of waste from care activities involving risk of infection (DASRI).
Enforce and monitor the obligation to compost or recover bio-waste.
Measures ‘by reduction objectives'
These are emissions linked to medicines and medical devices. Current knowledge does not allow us to precisely quantify the decarbonisation potential of these items. An initial GHG emissions reduction target has been set for 2050. This can be achieved by applying a two-pronged approach: on the one hand, reducing the volumes of consumables used, and on the other, reducing the carbon intensity of healthcare industries (a target of 60% has been set here, which means that the industry will have to produce the same unit of drugs or medical devices while emitting 60% less greenhouse gases).
Medicines (-63% of emissions from purchases of medicines, i.e. 9.6 MtCO2e)
The proposed measures are as follows:
Make the granting or renewal of Marketing Authorisation (MA) conditional on publication of the drug's carbon content.
Implement an eco-responsible purchasing policy (for all equipment and services) and make the carbon footprint of each product mandatory and decisive in calls for tender.
Partially relocate certain essential molecules to Europe. This must be accompanied by a thorough decarbonisation of manufacturing and distribution processes9.
Reduce the use of medicines and the quantity of unused medicines.
Medical devices (-67% of emissions from purchases of medical devices, i.e. 7.2 MtCO2e)
The proposed measures are as follows:
Making the issue or renewal of CE marking conditional on publication of the carbon content of the medical device. The industry will have to carry out an in-depth decarbonisation of its manufacturing and distribution processes.
Implement an eco-responsible purchasing policy (for all equipment and services) and make the carbon footprint of each product mandatory and decisive in calls for tender.
Involve professionals and learned societies in adapting practices that consume less medical equipment and materials, reflecting on the relevance of improving quality/safety/financial versus carbon costs.
Reduce the use of medical devices and encourage the reuse of medical devices whenever possible. Question the use of single-use devices in all specialities by professionals in conjunction with their learned societies.
Simply decarbonising existing facilities will not be enough
After application of the proposed measures, the carbon footprint of the healthcare system in 2050 is estimated at more than 35.7 MtCO2e in the absence of any reduction in the carbon intensity of the drugs and medical devices industries. This footprint could be reduced to 19 MtCO2e if these industries managed to reduce their carbon intensity by 60%, while reducing the volumes of drugs and medical devices by 10% and 20% respectively. This would fall short of the target of reducing emissions by 80% by 2020, equivalent to around 10 MtCO2e.
This clearly shows that, all other things being equal, an isolated decarbonisation strategy, even a very ambitious one, will not be enough to bring about a turnaround in the sector that is commensurate with the environmental challenges.
This points to the need for a more profound transformation of our business models in order to reduce the demand for upstream care. In other words, it is imperative to combine decarbonisation with policies of prevention, health promotion and fair care.
This is the subject of the final part of this course, which will explore the opportunities offered by a paradigm shift based on a consideration of health-environment co-benefits.